Qinlock—engineered to block the drivers of resistance in advanced GIST1,2
Qinlock is the first and only switch-control kinase inhibitor that provided broad-spectrum inhibition of KIT and PDGFRA kinase signaling in vitro through a novel dual mechanism of action1,2*
Voiceover:
How QINLOCK Works
Gastrointestinal stromal tumor, or GIST, is often driven by primary activating mutations in kinase genes KIT and PDGFRA.
70% to 80% of GIST have mutations in one or more regions, or exons, of the KIT gene. 5% to 10% of GIST have mutations in the PDGFRA gene, and 10% to 15% of GIST are without mutations in KIT or PDGFRA genes. These are often referred to as wild type.
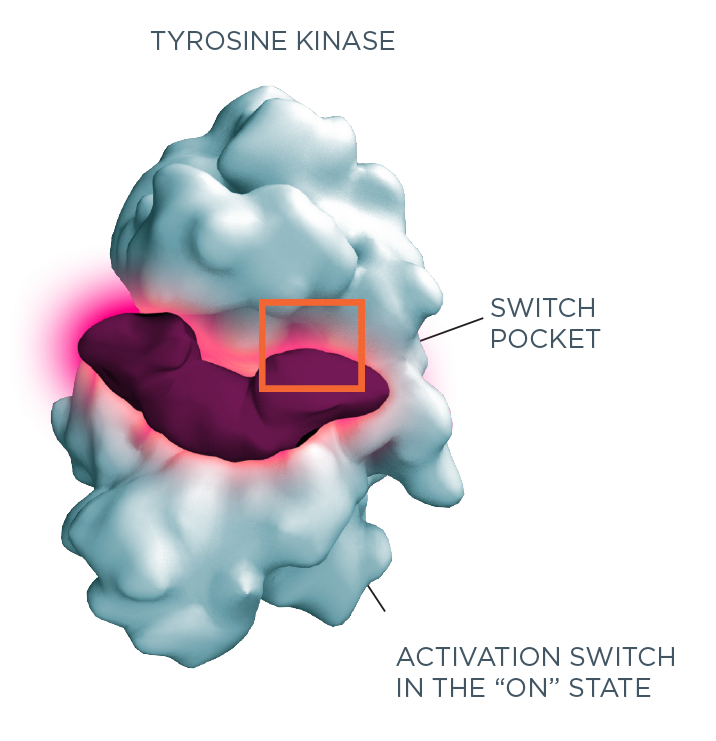
Kinase activation requires the interaction of two critical regions: the activation switch, and the switch pocket.
Mutations in tyrosine kinases, such as KIT or PDGFRA, cause uncontrolled interaction of the activation switch with the switch pocket.
This activates the kinase and leads to upregulation of kinase signaling, which drives cancer cell proliferation and/or survival.
As secondary drug-resistance mutations emerge, some tyrosine kinase inhibitors may lose their ability to prevent kinase activation, leading to cancer cell proliferation, otherwise known as drug resistance.
Complicating treatment even further, following failure of frontline TKI therapy, GIST patients often have multiple tumors, each of which can be driven by different secondary mutations.
The QINLOCK mechanism of action.
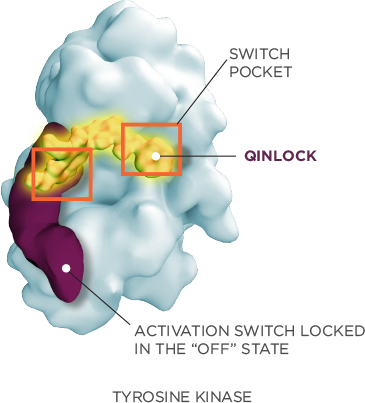
QINLOCK is a novel switch-control kinase inhibitor that provides broad-spectrum inhibition of KIT and PDGFRA kinase signaling in vitro through a dual mechanism of action.
As shown in preclinical studies, QINLOCK binds to both the activation switch and switch pocket and locks the kinase in the inactive state. This dual mechanism of action has been shown to potently inhibit kinase activation across the broad spectrum of mutations in KIT and PDGFRA kinases known to drive drug resistance and disease progression in advanced GIST.
Kinase activation requires the interaction of two critical regions2,3:
- Activation switch
- Switch pocket
As shown in preclinical studies, Qinlock1,2*
-
BINDS
to both the activation switch and switch pocket, regardless of where mutations arise -
LOCKS
the kinase in the inactive ("off") state, inhibiting downstream signaling and cancer cell proliferation
In vitro studies not designed
to assess clinical efficacy
In preclinical studies, this dual mechanism provided broad‑spectrum inhibition of KIT and PDGFRA kinase activity, including1*:
- Multiple primary mutations
- Multiple secondary mutations
- Wild type
*In vitro studies not designed to assess clinical efficacy.
Qinlock was studied in a global, randomized, Phase 3 trial1
The patient population of the INVICTUS trial was the most heavily pre-treated cohort ever studied in a Phase 3, randomized 4th-line GIST setting4
Once-Daily Dosing
Qinlock is dosed orally, once daily, with or without food1
Dosing & AdministrationView the Safety Profile
The rates of Grade 3/4 adverse reactions were similar between Qinlock and placebo5
View Qinlock Safety